Intraocular Drug Delivery System.
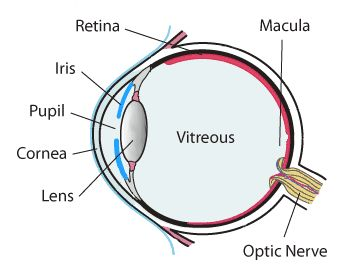
The anatomy and physiology of the eye are complex and distinct.
The anterior segment and the posterior segment are the two main components of the eye's structure.
About one-third of the eye is made up of the anterior segment, and the rest is made up of the posterior segment.
The anterior portion is made up of tissues such as the cornea, conjunctiva, aqueous humor, iris, ciliary body, and lens.
Sclera, choroid, retinal pigment epithelium, neural retina, optic nerve, and vitreous humor comprise the posterior segment of the eye.
Several vision-threatening diseases affect the anterior and posterior segments of the eye.
Diseases affecting the anterior segment include, but are not limited to glaucoma, allergic conjunctivitis, anterior uveitis, and cataract.
The most common diseases affecting the posterior segment of the eye are age-related macular degeneration (AMD) and diabetic retinopathy.
Ocular administration of the drug is primarily associated with the need to treat ophthalmic diseases.
The eye is the site for topical medication administration.
The primary goal of ophthalmic drug delivery is to sustain drug release and remain in the vicinity of the front of the eye for an extended period of time.
There are specialized dosage forms designed to be instilled into the eye's external surface (topical), administered inside (intraocular) or adjacent to the eye (periocular), or used in conjunction with an ophthalmic device.
Ocular Drug Delivery System is a novel approach to drug delivery in which the drug is instilled in the cul de sac cavity of the eye (space between the eyelids and eyeballs).
Solutions, suspensions, and ointments are the dosage forms that are used the most frequently.
The most recent dosage forms include implants, gels, gel-forming solutions, ocular inserts, and intravitreal injections.
Chemical Composition of the Eye:
Eye is composed of
Water - 98%,
Solid - 1.8%,
Protein - 0.67%,
Sugar - 0.65%,
NaCl — 0.66%,
Other mineral elements Sodium, Potassium and Ammonia - 0.79%.
Mechanism of Ocular Absorption.
Non-Corneal Absorption:
The penetration is through the Sclera and Conjunctiva into the intraocular tissues.
It is ineffective because it prevents the drug from entering the aqueous humor.
Corneal Absorption:
The outer epithelium has a rate-limiting barrier with pore size 60 Å that allows only small ionic and lipophilic molecules to pass through.
Trans-cellular transport occurs between the corneal epithelium and the stroma.
Drugs absorbed through corneal discharge into the systemic circulation via aqueous humor.
Factors Affecting Intraocular Bioavailability.
Lacrimal fluids.
Naso-lacrimal drainage.
Interaction of drugs with proteins of lacrimal fluids.
Dilution with tears.
Cornear barriers.
Active ion transport at the cornea.
Ophthalmic Dosage forms.
Ophthalmic dosage forms are sterile products that have been appropriately compounded and packaged for administration into the eye.

Advantages of Ocular Drug Delivery System:
It can be easily administered.
They have quick absorption and effect.
Less visual and systemic side effects.
Better patient compliance.
It provides a sustained and controlled drug delivery system.
Accurate dosing.
Disadvantages of the Ocular Drug Delivery System:
Shorter residence time of the drug at the eye surface.
Bioavailability is low.
The dissolved drug's instability.
Because of the low concentration of preservatives, the shelf life after opening the bottle is reduced.
Dosage form cannot be terminated during an emergency.
It interferes with vision.
It is difficult to place and remove.
There is occasional loss during sleep or while rubbing eyes.
Ideal Characteristics of Ocular Drug Delivery System:
It must be sterile.
It should be isotonic with respect to body fluids.
pH/buffer adjustment
Less prone to drainage.
Protein binding to a minimum.
Barriers to Ocular Drug Delivery System.
The presence of numerous barriers is the main factor contributing to the difficulty in achieving therapeutic doses that are relevant within the eye.
Before a dosage form reaches its site of action when it is applied topically or systemically, it must overcome numerous challenges.
As a result, only 1%–7% of the applied dose of drugs administered topically are typically bioavailable to the eyes.
Anatomical barriers and physiological barriers are two broad categories for these barriers.

Image Source: https://www.researchgate.net/profile/Prakash-Bisen
Anatomical Barriers:
There are two entry points for a dosage form when applied topically: either through the cornea or another route.
The cornea is made up primarily of five sections and is a very tight, multilayered tissue.
Hydrophilic drug transport through intercellular spaces across the epithelium-principle barrier.
Bowman's membrane.
Stroma-multiple layers of collagen fibers containing pores and channels (for lipophilic drug, significant barrier).
Descemet’s membrane.
Endothelium.
Prevention: Proper lipophilicity and hydrophilicity ratios for maximum bioavailability.
The non-corneal route moves over the conjunctiva and sclera while avoiding the cornea.
Conjunctiva: It is more permeable to hydrophilic molecules than the cornea.
2. Physiological Barriers:
The tear film is the eye's main line of defense.
Precorneal factors like solution drainage, tear dilution, tear turnover, and increased lacrimation further reduce the bioavailability of drugs that are applied topically.
The exact time for absorption is subsequently shortened, which reduces bioavailability.
Prevention:
To avoid significant precorneal loss, medications used as eye drops must be isotonic and non-irritating.
3. Blood Ocular Barrier:
Normally, this barrier prevents most drugs from entering the eye, but inflammation causes this barrier to dissolve, allowing drugs and large molecules to enter the eye.
Blood aqueous barrier:
The ciliary epithelium and capillaries of the iris.
Blood retinal barrier:
Tight junctions between retinal epithelial cells and non-fenestrated capillaries of the retinal circulation block the entry of large molecules from the choriocapillaris into the retina.
4. Drug and Dosage Form Related Factors:
Solubility:
Solubility is dependent on the pKa of the drug and the pH of the solution.
Lipophilicity:
Lipophilicity and corneal permeability display a sigmoidal relationship.
This is because of the differential permeability of the different layers of cornea towards lipophilic drugs.
Lipophilic drugs tend to permeate easily through the epithelial layers of the cornea and the hydrophilicity of the inner layer of the cornea (stroma) requires higher hydrophilicity for optimal permeation.
Molecular weight and size:
The weight and size of molecules play a critical role in deciding their overall permeability through the paracellular route.
Molecules having a molecular weight less than 500 Dalton can permeate readily.
The conjunctiva has a larger paracellular pore diameter thus allowing permeation of larger molecules such as small and medium-size peptides (5000-10000 Daltons).
Permeation across the sclera occurs through the aqueous pores and the molecular size of the solute can be the determining factor.
Sucrose (molecular weight - 342 Daltons) permeates 16 times faster than inulin (molecular weight - 5000 Daltons).
Scleral permeability is approximately half of the conjunctiva but much higher than the cornea.
Methods to Get Around Obstacles in Ocular Drug Delivery.
The success of drug delivery via topical or systemic routes is constrained by a number of issues.
Drug design, drug formulation, and device innovations have produced successful products. But scientists have experimented with alternative drug delivery methods that can get around problems caused by the more traditional ones.
A skilled professional routinely administers injections to various parts of the ocular structures through the visible portions of the sclera.
Some of the important methods are discussed here as follows,
Intravitreal Injections.
Intravitreal Injections.
Retrobulbar and Peribulbar Route.
Sub-Tenon Injections.
Intracameral Injections.
Intravitreal Injections:
Intravitreal injection (IVI) involves delivering the drug formulation directly into the vitreous humor through pars plana.
This procedure avoids the cornea and the scleral blood vessels while providing direct access to the vitreous.
Formulations such as; solution, suspension, or a depot formulation can be administered through this route.
After a first-order rate of decline, drug elimination occurs through the retina or the anterior chamber via the aqueous humor.
The relationship between this rate of elimination and the drug's molecular weight is linear. Larger molecules typically have half-lives that can reach several weeks as opposed to low molecular weight compounds, which typically have half-lives of less than 3 days.
The administration is linked to side effects like endophthalmitis, hyperemia, and retinal detachment.
In order to improve patient compliance, sustained release drug delivery systems can help by reducing the frequency of administration.
Subconjunctival Injections:
Under the conjunctival membrane that lines the inner surface of the eyelid, this injection places the medication.
The drug can now have direct access to the sclera by avoiding the cornea and conjunctiva.
Compared to intravitreal injections, it is significantly less invasive and has fewer side effects.
The technique is a great way to deliver hydrophilic medications because it gets around their rate-limiting barriers and allows more medication to enter the vitreous.
It is a great way to deliver macromolecular medications like insulin and Avastin (bevacizumab, a recombinant monoclonal antibody against VEGF), as well as depot-forming formulations.
Retrobulbar and Peribulbar Route:
A retrobulbar injection delivers the medication to the retrobulbar space through the orbital fascia and eyelid.
Using this method, medications like antibiotics and corticosteroids are delivered to the back of the eyeball.
The delivery of anesthetic agents can be done particularly well using this route.
However, it is a very delicate procedure that needs the right training and tools because it could harm the optic nerve.
Drug delivery via the peribulbar route involves injections above and/or below the globe.
It is also a practical method for administering anesthesia, particularly when performing cataract surgery.
When compared to the retrobulbar route, it is safer and less dangerous.
Although it is a safer procedure, numerous cases of elevated intraocular pressure following peribulbar injections have been documented, in contrast to retrobulbar injection.
Sub-Tenon Injections:
A blunt cannula is used to administer sub-tenon injections into the space between the tenon's capsule and sclera.
Additionally, deep sedation prior to surgery is not necessary for this procedure.
Compared to retrobulbar and peribulbar administration, the sub-tenon route for administering anesthesia appears to be safer and more effective because it does not call for sharp needles.
Additionally, uveitis, cystoid macular edema, complicating uveitis, and non-necrotizing scleritis have all been successfully treated with steroids injected through this route.
Intracameral Injections:
Similar to intravitreal injections, intracameral injections deliver medication to the anterior chamber.
The anterior chamber is the only place where medications can be delivered through this route, with very little access to the posterior segment.
Typically, it is used in anterior segment procedures like cataract surgery.
Dexamethasone administered intracamerally is effective in reducing postoperative inflammation in both glaucomatous and non-glaucomatous patients, according to clinical studies.
Compared to topical antibiotics and antifungal agents, it is an effective and frequently more affordable method of delivering antibiotics.
Formulations for Ocular Drug Delivery System.
Conventional Delivery Systems
Eye drops
Gels and ointments.
Ocuserts & Lacriserts
Vesicular Systems
Liposomes
Niosomes and Discomes (Giant Niosomes)
Controlled Delivery Systems
Implants
Iontophoresis
Dentrimer
Microemulsion
Nanosuspension
Microneedle
Mucoadhesive Polymers
Ocular Inserts:
They can be classified as follows,
Non-Erodible Inserts:
Ocusert
Contact Lens
Erodible Inserts:
Lacriserts
SODI
Mindisc
Non-Erodible Inserts:
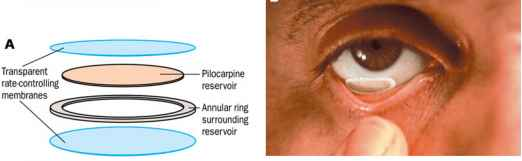
Ocusert:
It is a flat, flexible, elliptical device designed to be placed in the inferior cul-de-sac between the sclera and eyelid which releases Pilocarpine continuously at a steady state for 7 days.
It comprises of 3 layers:
Outer Layer: Ethylene-vinyl acetate copolymer layer.
Inner Layer: Pilocarpine gelled with alginate main polymer.
A retaining ring of EVA impregnated with titanium dioxide.
Example: Pilo 20 (20 mg/hr), Pilo 40 (40 mg/hr).
Contact Lens:
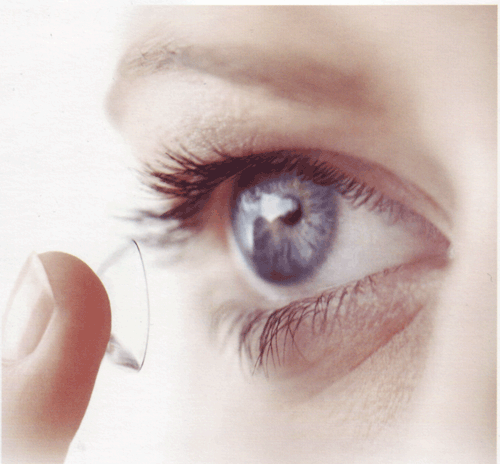
These circular structures might have dyes added while they are being polymerized.
Whether a drug is incorporated depends on the structure's hydrophilicity or hydrophobicity.
2. Erodible Inserts:
Lacriserts:

It is a sterile, HPC-based, preservative-free device in the form of a rod.
Its dimensions are 12.5 mm in diameter, 3.5 mm in length, and 5 mg in weight.
It is applied in the Keratitis Sicca treatment of dry eyes.
SODI (Soluble Ocular Drug Insert):
placed in the lower fornix.
It is a tiny, acrylamide vinyl pyrrolidone and ethyl acrylate-based insert that dissolves in water.
It has a weight of 15–16 mg, a softening time of 10–15 seconds, a viscous liquid time of 10–15 minutes, and a polymeric solution time of 30–60 minutes.
Both trachoma and glaucoma are treated with it.
Minidisc:
It consists of a counter disc that touches the eyeball and has a convex front and concave back.
It measures 4-5 mm in diameter.
It has a diameter of 4-5 mm.
E.g. Pilocarpine, Chloramphenicol.
Commonly Asked Questions.
Discuss the Intraocular Drug Delivery System in detail.
Write a note on novel approaches for drug delivery to the eye.
Labels: NDDS


<< Home